
- Birth Injury Errors
- Brain Damage/Brain Injuries
- Cancer
- Dialysis Mistakes
- Eye Cases
- Gastroenterology
- Heart Disease and Attacks
- Infections and Infectious Diseases
- Internal Medicine/Primary Care
- Medication Errors
- Pulmonary and Respiratory Diseases
- Radiology/Diagnostic Testing
- Retained Instrument/Sponge Cases
- Skeletal Injuries
- Spinal Cord Injuries
- Strokes
- Surgery and Procedures
- Traumatic Injuries
- Urology
- Vascular Injuries and Diseases
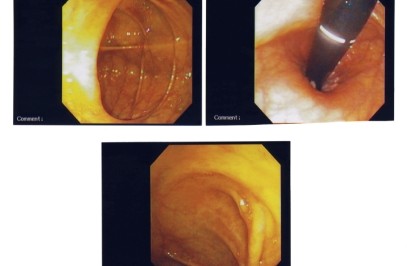
Colonoscopy
Colonoscopy is an endoscopic examination of the colon and the distal part of the small bowel. It is performed with a flexible tube with a camera on the end which is passed through the anus. It allows the GI physician to make a visual inspection and diagnosis of the colon and small bowel to determine if ulcerations or polyps exist. It also allows the opportunity for a biopsy or removal of tissue for closer examination under a microscope to determine if they are precancerous.
Colonoscopy allows for the examination of the entire colon, which measures four to five feet in length. Indications for a colonoscopy include:
-
Rectal bleedingBlood in the stool
-
Unexpected changes in bowel habits
-
Age 50 years.
A colonoscopy should be performed on all patients age 50 years or greater as a routine examination regardless of a family history of colon cancer or symptoms. Preparation for a colonoscopy includes a cleansing of the colon of all fecal matter on the night before the procedure. This will usually involve a laxative preparation such as polyethylene glycol. Often the preparation will involve both a pill form laxative and a bowel irrigation preparation (enema). For one to three days before the procedure, the patient is required to follow a clear liquid diet. This would include the liquids of apple juice, chicken or beef broth, lemon-lime soda (Sprite or 7up), Gatorade or Powerade and water. Fluids such as orange juice prune juice and milk should be avoided. In most cases black coffee is allowed.
The physician will usually ask patients to forego Aspirin and other blood thinners for a period of ten days before the procedure. Ask your physician if you are on blood thinners. On the day of the procedure, the patient is given sedation intravenously. Fentanyl or midazolam are usually used, but Demerol may be used as an alternative. The patient is then positioned on the examination table on his left side and the endoscope is passed through the anus, up the rectum and colon and ultimately the terminal ileum. In most instances , the entire procedure takes about 20-30 minutes. More than half of that time is usually spent withdrawing the endoscope and closely inspecting for polyps or other suspicious masses.
If a polyp is identified, a sterile solution is injected under the polyp to lift it away from the deeper tissues. The polyp is then removed with instruments placed in the endoscope. It will be sent to the laboratory for closer microscopic inspection. Suspicious lesions may also be cauterized with laser light or cut with an electric wire. Medications can also be injected to control the bleeding of the lesions when they are cut.
Outpatient recovery time may range from 30-6o minutes. Most facilities require that patients have a person to drive them home after the procedure because of the sedatives. Although colonoscopy is a safe procedure, complications are estimated to occur approximately 0.5 percent of the time. Some of the known complications include perforation, or a tear or hole in the intestine. This can occur when the endoscope is being maneuvered through some of the sharp turns of the colon. Bleeding is another known complication and occurs in 1 out of every 1000 procedures. Infection is another risk of this procedure.
According to the Annals of Internal Medicine, the rate of serious complications from colonoscopy screening for cancer is “10 times higher than for any other commonly used cancer-screening test.” Thus, you should carefully consider the risks and benefits of colonoscopy before agreeing to undergo this procedure.




